|
At the beginning of my project, I was completely unsure of what I wanted to do after my BASIS career. I always thought I would go to college to pursue a finance degree, but medicine was always a subject that I was really interested in. After completing my project, I have learned so much about how doctors interact with patients, and how they both collaboratively decide on how to maintain health. Because of my project, I have become so much more intrigued in this field, and I plan on studying both finance and medicine in college. Thank you all for reading my blog, and my project couldn't have been done without the help from Mrs. Streuber and Dr. Shakil.
1 Comment
 If you watch TV, you may have seen ads like Advil and Aleeve, which promote the daily use of their pain-relieving products. These pain medicines are unique in the sense that they don’t require prescriptions, but many people don’t know that these can actually hurt the kidneys. In one of my first blogs, I explained that Dr. Shakil always asks patients if they take these pain medications, specifically Advil. The reason he does it is because if too many are taken in a day, it could significantly reduce kidney function. Many people are unaware of this, and as a result they take too many pills without knowing the dangerous risk they are taking. According to the National Kidney Foundation, approximately 3-5% of new patients diagnosed with kidney failure are due to the overuse of such pain medications.
When I first read this statistic, I was pretty confused. How much is “too much,” and do the labels not make it clear that your kidneys are at risk? I asked Dr. Shakil about the exact dosage kidney patients should take, if they should be taking any at all. He explained that the maximum dosage that is generally safe for regular people is 800 milligrams. For kidney patients, this dosage is extremely harmful and could cause a lot of damage. If patients are having a lot of pain, it is ok to prescribe 200-400 milligrams once a day. Overall, it is better to avoid these medications for daily use. As shown in the picture, the label on the back of the Advil bottle does not mention the harm it can do to your kidneys. Since this is an over-the-counter medication, it is allowed to be more lenient on what the label says. Prescription medications, on the other hand, are thoroughly tested by the FDA, so everything must be clear on the label. If too many of these pain medications are taken, then papillary necrosis will occur. This happens when blood flow is constricted to the outer parts of the kidneys, and the tissues slowly begin to die. Sources: "Analgesic Nephropathy." WebMD. WebMD, n.d. Web. 25 Apr. 2017. <http://www.webmd.com/a-to-z-guides/analgesic-nephropathy>. "Renal Papillary Necrosis." American Urological Association - Renal Papillary Necrosis. N.p., n.d. Web. 25 Apr. 2017. <https://www.auanet.org/education/modules/pathology/kidney-lesions/papillary-necrosis.cfm>. 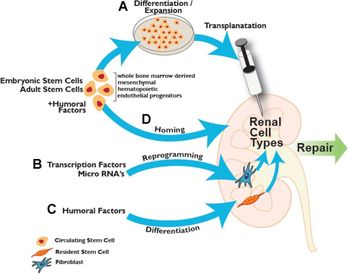 What if instead of having a donor, the patient themselves can remove stem cells from their own body to regenerate a brand new kidney? This may seem like science fiction, but researchers are trying to make this possible. Scientists are looking into how stem cells found in bone marrow can actually be reprogrammed into kidney cells, so that the kidney may be kept healthy and active.
Harvard’s stem cell institute has been the most successful so far. Their research is based off of mesenchymal stem cells, which are found in bone marrow. These stems cells act as the natural defense in the body, as they help to heal the kidneys if injured. These researchers are attempting to remove the proteins found in these cells and implement them into the kidney through transplantation, as shown in the picture. These cells may also be placed into dialysis machines, so the cells may go directly to the damaged kidneys. These stem cells are also being formed into specific kidney structures for long-term use. Nephrons located in the kidney, for example, filters blood and removes waste so it may be removed through urination. These Harvard scientist are attempting to mold these cells into the shape of a nephron, which will act out the functions of a real nephron. With this, the cells may be more effective in helping the kidneys with their normal functions. Sources: Herrera, Marcela, and Maria Mirotsou. "Stem cells: potential and challenges for kidney repair." American Journal of Physiology - Renal Physiology. American Physiological Society, 01 Jan. 2014. Web. 05 Apr. 2017. <http://ajprenal.physiology.org/content/306/1/F12>. "Kidney Disease." Harvard Stem Cell Institute (HSCI). Web. 05 Apr. 2017. <http://hsci.harvard.edu/kidney-disease-0>. "UNC Kidney Center." Parts of the Nephron - UNC Kidney Center. N.p., 29 June 2015. Web. 05 Apr. 2017. <http://unckidneycenter.org/images/kidney-health-library-pictures/parts-of-the-nephron/view>. Going back to last weeks blog, a kidney transplant is generally the best option for a patient with end-stage renal disease. Even though this is a life saving procedure, there are still many ethical questions to consider. The first ever kidney transplant occurred in 1954, and since then researchers have been improving the procedure to keep these kidneys lasting longer. As a result certain problems have arose, such as when to remove the kidneys when a patient dies, and when to declare him or her dead. Starting from the late 1960’s, laws were put in place to help those who want to donate their organs when they die, and to prevent the direct purchasing of kidneys to the patient.
Since these laws were passed many began to donate their kidneys, however this number is still not high enough. Every year the wait list keeps growing, and many die because they couldn’t find a match in time. As of January 2016, there are 100,791 patients waiting to receive a lifesaving kidney, and 3,000 new patients are added each month. In order to save more lives, should incentives be given to those who choose to donate? According to the US National library of medicine, many of those who need kidneys may go abroad, because they may be desperate to find a kidney quickly. As a result, many of these patients don’t question where the kidney itself comes from. Unfortunately, it has been found that many kidney donors in foreign countries donate so they can pay off debt to other people, and not just for charity. These donors also come from impoverished areas, where they are in need of money. Selling a kidney may not completely help out the financial situation of some. Many in fact still remain impoverished, as the debt they need to pay becomes too high. Does being paid to donate a kidney bring in more potential donors? Maybe. However, the health of both parties should be examined to make an accurate call. The kidney may help to save a life, but losing that kidney may not solve the problems of the donor. With money being thrown into the process in the United States, we may see the same result that has risen in foreign countries: a black market that feeds of the poor that only benefits certain people. Sources: "The President's Council on Bioethics: Organ Transplantation: Ethical Dilemmas and Policy Choices." The President's Council on Bioethics: Organ Transplantation: Ethical Dilemmas and Policy Choices. N.p., n.d. Web. 05 Apr. 2017. <https://bioethicsarchive.georgetown.edu/pcbe/background/org_transplant.html>. Adair, Anya, and Stephen J. Wigmore. "Paid organ donation: the case against." Annals of The Royal College of Surgeons of England. The Royal College of Surgeons of England, Apr. 2011. Web. 05 Apr. 2017. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3291132/> "Organ Donation and Transplantation Statistics." The National Kidney Foundation. N.p., 11 Jan. 2016. Web. 05 Apr. 2017. <https://www.kidney.org/news/newsroom/factsheets/Organ-Donation-and-Transplantation-Stats>. 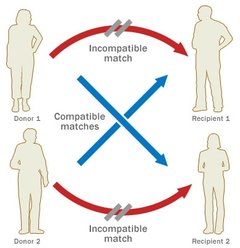 When the patient reaches end-stage renal disease they are usually faced with two options: dialysis or a transplant. Dialysis is the more common of the two, but transplants may keep the patient more free and independent. There are two main types of kidney procedures: deceased-donor and living-donor transplants.
A healthy individual has the option to donate his or her body when they die, and the kidneys are often utilized in transplants. Once the kidney is removed from the deceased body, it is either iced immediately, or is kept on a machine that pumps oxygen into the tissues so it may remain healthy and fresh. Either way, it is crucial that the kidney does not travel very far, because the more time spent outside a living body the worse it may become. Contrary to popular belief, a patient with end-stage renal disease only needs one kidney, so thankfully resources may be saved. The non-functioning kidney still remains in the body, and the new kidney is placed in the front of the stomach, opposed to the back. This seems like a much better option than dialysis, because the patient doesn’t have to spend 12 hours a week in the clinic. However it is difficult to find a match for a patient, due to the lack of compatibility and registered donors. About two thirds of transplant patients receive kidneys from deceased donors, whereas the others mostly come from live donors. Generally speaking, living-donor kidneys do much better than deceased kidneys. For one, the kidney lasts longer both in the short term and the long term. Deceased donor kidneys may also have delayed functions, whereas the living donor kidney starts working immediately. If you wanted to donate your kidney to a close friend or family member, it is important to know what makes a good “match.” No two individuals are the exact same: we each have different blood and tissue types. They do not have to be the exact same, but the blood must be compatible. For example, if the donor is blood type A, they are compatible with patients who have blood types AB and A. But even if you aren’t exactly compatible with the person you want to donate to, there is still a way for it to work! The transplant clinic may offer you and the patient a chance to do a paired donation. As shown in the diagram, your blood and tissue types are compared with other patients in the clinic, and if you can match with a patient who couldn’t match with their preferred donor, the two donors may “trade” kidneys to make both patients happy. Donors are unfortunately very scarce, but due to the amount of people needing kidneys, you will most likely find a patient that matches with your kidney, so it will not be wasted. Sources: Mayo Clinic Staff Print. "Kidney Transplants." Mayo Clinic. N.p., 24 June 2016. Web. 03 Apr. 2017. <http://www.mayoclinic.org/tests-procedures/living-donor-kidney-transplant/pdc-20207271>. "Organ Donation: Demand versus Supply." ExpatHealth.org. N.p., n.d. Web. 03 Apr. 2017. <https://expathealth.org/healthcare-news/organ-donation-demand-versus-supply/>.  Many patients come in to Dr. Shakil’s clinic with diabetes or high blood pressure, and while these are the two most common reasons for Chronic Kidney Disease, they are others who come with rare conditions. Last week I met a patient who suffered from glomerulonephritis, or simply inflammation of the blood vessels in the kidneys. I asked Dr. Shakil for clarification on the matter, and he explained that there are a lot of different causes for inflammation. This specific patient suffers from systemic lupus erythematosus, an autoimmune disease that attacks certain organs in the body. In the patient's case, the kidneys were being attacked by her own immune system, which caused the inflammation. In most cases this inflammation can easily go away without treatment, with the patient we saw treatment had to take place, to avoid damage in the kidneys. The patient showed signs of Chronic GN, because excess protein was found in the urine, and the lower parts of her legs were very swollen. To counter these symptoms, Dr. Shakil put the patient on certain corticosteroids, to suppress the immune system. It is also important for the patient to reduce their intake of salt and protein. As shown in the picture above, Lupus can do extensive harm to the kidneys if not treated. If you have this condition, it is extremely important to check regularly with a doctor, as it can harm not only the kidneys, but other organs as well. If left untreated, the inflamed kidney may end up like the one on the right Sources: Hassan, Saloni Editorial Head Umair. "Nephritis – Symptoms, Causes and Home Remedies." Saloni Health & Beauty Supply. N.p., 22 Sept. 2014. Web. 27 Mar. 2017. <https://makeup.saloni.pk/2014/09/22/nephritis-symptoms-causes-and-home-remedies/>. Written by Christine Case-LoMedically Reviewed by. "Glomerulonephritis." Healthline. N.p., n.d. Web. 27 Mar. 2017. <http://www.healthline.com/health/glomerulonephritis#Symptoms3>. 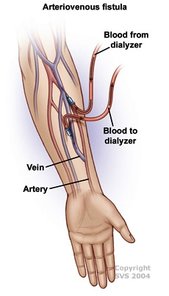 The fistulas themselves are fairly complicated, because there are several types that are installed for different reasons. A fistula is defined as a surgical passage that connects two “hollow” organs. There are three main types of fistulas that may be used for dialysis: Arteriovenous fistulas, arteriovenous grafts, or venous catheters.
In the case of a dialysis fistula (as shown on the left), an artery is attached to the vein in the arm, and maturation of the fistula is necessary. It takes around three- six months for this fistula to mature, so if the patient is becoming close to dialysis, it is important for them to get this surgery. This is the most preferred way to get a fistula, as it has the lowest infection rate. However if the patient has small veins, they must consider other options. Grafts are normally placed if fistulas cannot be created. Instead of the artery being attached to the vein by surgery, an artificial tube made from fabric is added. The tube is put underneath the skin, and when it is time for dialysis, it will be attached to the machine. Arteriovenous grafts tend to last two to three years due to persistent clotting. Many patients I saw at the dialysis center had venous catheters, which are inserted in a large vein in the neck. A large portion of the catheter remains outside the body so it can be easily attachable to a dialysis machine, and as a result it may become easily infected. Sources: "Dialysis." Dialysis. N.p., n.d. Web. 21 Mar. 2017. <http://vascularim.com/dialysis.php>. "Vascular Access, Arteriovenous Fistula, Arteriovenous Graft, Venous Catheter." Department of Surgery. N.p., n.d. Web. 21 Mar. 2017. <http://www.surgery.usc.edu/vascular/vascularaccess.html>.  Going back to my very first blog post, Chronic Kidney Disease is comprised of five different stages, each representing the percentage of kidney function that is left. But what options does the patient have if the kidneys are no longer functioning? If the nephrologist concludes there is no recovery possible, he/she will recommend the patient go on dialysis. Dr. Shakil will take several steps early on to avoid dialysis, because it is very costly and time consuming for the patient. However once the patient has little kidney function remaining, there are three options that are available: Hemodialysis, peritoneal dialysis, and hemofiltration.
I went to the Kingman Dialysis Center to check out what dialysis is really like. Once inside the building, you will see a large room filled with armchairs and dialysis machines. There are around 15-20 patients at the center at a time, and the process normally takes around four hours a day for three days a week. In the back of the center, out of sight from the patients, is the room where the chemicals are synthesized. Each patient is attached to a large machine, as shown below. The main job of this machine is to take the unfiltered blood out of the body, and it reenters the body after the toxins have been removed. It sounds simple, but the machine itself is fairly complicated. There are normally two jugs that are in front of the machine. One of the jugs mixes the unfiltered waste with an acidic solution, that contains electrolytes and minerals which help keep the patient healthy. The other jug contains a bicarbonate solution, that goes into the machine and mixes with purified water. The two solutions found in these jugs are the same solutions being synthesized in the back! Once the blood is cleansed with the chemicals, they re enter the body. Once this process is over, an alarm will sound, which notifies the patient that the process for the day has been completed. Next week I will explain how the tubes are placed in the arm, along with the surgery that needs to take place so they may remain safely in the patient. Source: "Hemodialysis." The National Kidney Foundation. N.p., 14 Feb. 2017. Web. 12 Mar. 2017. <https://www.kidney.org/atoz/content/hemodialysis>. Along with Polycystic Kidney Disease and Diabetes, simple kidney stones can cause real harm as well. Dr. Shakil explained to me that when high levels of oxalate and calcium are introduced into the kidneys, these minerals may start to crystallize, causing stones to form. Once stones form in the kidneys, the patient may start to see several symptoms, including pain in the sides and back, and unusual smell in the urine.
If the pain gets too unbearable, it is important to see a doctor right away, as stones may lead to more damage. Once the doctor confirms the patient has a kidney stone, several treatment options are available. For small stones that don’t cause much pain, many patients simply choose to pass the stone through simple urination. To do this, it is important for the patient to drink around two-three quarts of water a day. The doctor may also recommend weak pain relievers, such as Aleve or Advil. If the stone becomes too hard to pass, the doctor may prescribe an alpha blocker as well, which relaxes the muscles to help pass the stone without much pain or discomfort. But what happens when the stone is too large to pass? New advances in medicine have allowed shock wave therapy to come into play. The procedure known as extracorporeal shock wave lithotripsy, or ESWl, creates strong sound waves that break up the stone, so these smaller stones are able to pass through urination. If this procedure is unsuccessful, the stone may be removed surgically. These stones in general cause a lot of pain, but they can easily be prevented. Contrary to popular belief, it is important to eat calcium rich foods, as they can still easily pass through the kidney if a large amount is present. A diet low in salt and protein will help with prevention as well, as these may cause sodium to leak into urine. About one in ten people will have at least one kidney stone in their lifetime, so it is important to spread awareness in order to avoid this pain in the future. Source: "Kidney stones." Mayo Clinic. Web. 05 Mar. 2017. <http://www.mayoclinic.org/diseases-conditions/kidney-stones/basics/definition/con-20024829>. This week I saw several patients who were on dialysis, where an external machine filters out blood, which takes over the function of the kidneys. This process has been around for decades, and it has gone under many variations and changes to make it more efficient. The risks associated with dialysis have stayed the same as well, and even though it is rare, cysts may start to form. Polycystic Kidney Disease, or PKD, is when cysts filled with water-like fluid start to form around the outer edges of the kidneys. High blood pressure is very common with this disease. PKD is also considered to be a genetic disorder, as it is passed down through generations. There are two main types of inherited PKD: Autosomal Dominant and Autosomal Recessive. Autosomal Dominant is never found at an early stage in life, and as a result it is diagnosed when the patient is in adulthood. This type of PKD is especially concerning because symptoms do not appear until the cysts have grown to full length. Autosomal Recessive, on the other hand, is found within the few first months of life, so treatment may begin much earlier. Either way, cysts on the kidneys can cause liver failure, cardiovascular disease, kidney stones, and blindness. All of these conditions sound very difficult to deal with, but treatment is available to weaken these symptoms. It is important for the patient to be on blood pressure medication, as high blood pressure is fairly common with this disease. Pain medication is also necessary, but strong medications such as Aleve or Advil may cause further injury, due to restricted blood flow to the kidneys. Sodium levels need to be controlled as well, as high sodium levels cause damage as well. Kidneys also grow to abnormally large sizes once this disease progresses. If they become too large to the point where renal failure becomes possible, a transplant may be needed. The kidney on the right is healthy, whereas the one on the left has several cysts, and has grown to an unhealthy size. Sources: “ADPKD.” PKD International. 26 Feb. 2017 <http://www.pkdinternational.org/what-is-pkd/adpkd/>. "Polycystic Kidney Disease (PKD) | NIDDK." National Institutes of Health. U.S. Department of Health and Human Services. Web. 26 Feb. 2017. <https://www.niddk.nih.gov/health-information/kidney-disease/polycystic-kidney-disease>. 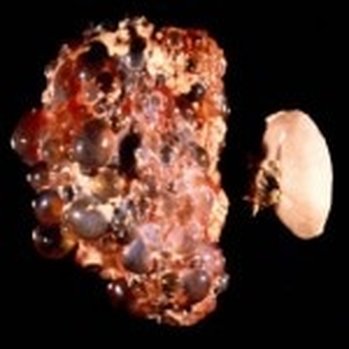 |
