 If you watch TV, you may have seen ads like Advil and Aleeve, which promote the daily use of their pain-relieving products. These pain medicines are unique in the sense that they don’t require prescriptions, but many people don’t know that these can actually hurt the kidneys. In one of my first blogs, I explained that Dr. Shakil always asks patients if they take these pain medications, specifically Advil. The reason he does it is because if too many are taken in a day, it could significantly reduce kidney function. Many people are unaware of this, and as a result they take too many pills without knowing the dangerous risk they are taking. According to the National Kidney Foundation, approximately 3-5% of new patients diagnosed with kidney failure are due to the overuse of such pain medications.
When I first read this statistic, I was pretty confused. How much is “too much,” and do the labels not make it clear that your kidneys are at risk? I asked Dr. Shakil about the exact dosage kidney patients should take, if they should be taking any at all. He explained that the maximum dosage that is generally safe for regular people is 800 milligrams. For kidney patients, this dosage is extremely harmful and could cause a lot of damage. If patients are having a lot of pain, it is ok to prescribe 200-400 milligrams once a day. Overall, it is better to avoid these medications for daily use. As shown in the picture, the label on the back of the Advil bottle does not mention the harm it can do to your kidneys. Since this is an over-the-counter medication, it is allowed to be more lenient on what the label says. Prescription medications, on the other hand, are thoroughly tested by the FDA, so everything must be clear on the label. If too many of these pain medications are taken, then papillary necrosis will occur. This happens when blood flow is constricted to the outer parts of the kidneys, and the tissues slowly begin to die. Sources: "Analgesic Nephropathy." WebMD. WebMD, n.d. Web. 25 Apr. 2017. <http://www.webmd.com/a-to-z-guides/analgesic-nephropathy>. "Renal Papillary Necrosis." American Urological Association - Renal Papillary Necrosis. N.p., n.d. Web. 25 Apr. 2017. <https://www.auanet.org/education/modules/pathology/kidney-lesions/papillary-necrosis.cfm>.
1 Comment
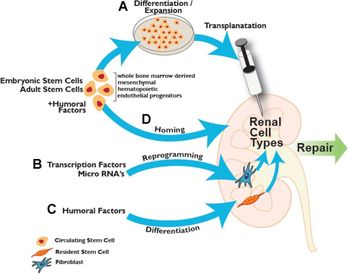 What if instead of having a donor, the patient themselves can remove stem cells from their own body to regenerate a brand new kidney? This may seem like science fiction, but researchers are trying to make this possible. Scientists are looking into how stem cells found in bone marrow can actually be reprogrammed into kidney cells, so that the kidney may be kept healthy and active.
Harvard’s stem cell institute has been the most successful so far. Their research is based off of mesenchymal stem cells, which are found in bone marrow. These stems cells act as the natural defense in the body, as they help to heal the kidneys if injured. These researchers are attempting to remove the proteins found in these cells and implement them into the kidney through transplantation, as shown in the picture. These cells may also be placed into dialysis machines, so the cells may go directly to the damaged kidneys. These stem cells are also being formed into specific kidney structures for long-term use. Nephrons located in the kidney, for example, filters blood and removes waste so it may be removed through urination. These Harvard scientist are attempting to mold these cells into the shape of a nephron, which will act out the functions of a real nephron. With this, the cells may be more effective in helping the kidneys with their normal functions. Sources: Herrera, Marcela, and Maria Mirotsou. "Stem cells: potential and challenges for kidney repair." American Journal of Physiology - Renal Physiology. American Physiological Society, 01 Jan. 2014. Web. 05 Apr. 2017. <http://ajprenal.physiology.org/content/306/1/F12>. "Kidney Disease." Harvard Stem Cell Institute (HSCI). Web. 05 Apr. 2017. <http://hsci.harvard.edu/kidney-disease-0>. "UNC Kidney Center." Parts of the Nephron - UNC Kidney Center. N.p., 29 June 2015. Web. 05 Apr. 2017. <http://unckidneycenter.org/images/kidney-health-library-pictures/parts-of-the-nephron/view>. Going back to last weeks blog, a kidney transplant is generally the best option for a patient with end-stage renal disease. Even though this is a life saving procedure, there are still many ethical questions to consider. The first ever kidney transplant occurred in 1954, and since then researchers have been improving the procedure to keep these kidneys lasting longer. As a result certain problems have arose, such as when to remove the kidneys when a patient dies, and when to declare him or her dead. Starting from the late 1960’s, laws were put in place to help those who want to donate their organs when they die, and to prevent the direct purchasing of kidneys to the patient.
Since these laws were passed many began to donate their kidneys, however this number is still not high enough. Every year the wait list keeps growing, and many die because they couldn’t find a match in time. As of January 2016, there are 100,791 patients waiting to receive a lifesaving kidney, and 3,000 new patients are added each month. In order to save more lives, should incentives be given to those who choose to donate? According to the US National library of medicine, many of those who need kidneys may go abroad, because they may be desperate to find a kidney quickly. As a result, many of these patients don’t question where the kidney itself comes from. Unfortunately, it has been found that many kidney donors in foreign countries donate so they can pay off debt to other people, and not just for charity. These donors also come from impoverished areas, where they are in need of money. Selling a kidney may not completely help out the financial situation of some. Many in fact still remain impoverished, as the debt they need to pay becomes too high. Does being paid to donate a kidney bring in more potential donors? Maybe. However, the health of both parties should be examined to make an accurate call. The kidney may help to save a life, but losing that kidney may not solve the problems of the donor. With money being thrown into the process in the United States, we may see the same result that has risen in foreign countries: a black market that feeds of the poor that only benefits certain people. Sources: "The President's Council on Bioethics: Organ Transplantation: Ethical Dilemmas and Policy Choices." The President's Council on Bioethics: Organ Transplantation: Ethical Dilemmas and Policy Choices. N.p., n.d. Web. 05 Apr. 2017. <https://bioethicsarchive.georgetown.edu/pcbe/background/org_transplant.html>. Adair, Anya, and Stephen J. Wigmore. "Paid organ donation: the case against." Annals of The Royal College of Surgeons of England. The Royal College of Surgeons of England, Apr. 2011. Web. 05 Apr. 2017. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3291132/> "Organ Donation and Transplantation Statistics." The National Kidney Foundation. N.p., 11 Jan. 2016. Web. 05 Apr. 2017. <https://www.kidney.org/news/newsroom/factsheets/Organ-Donation-and-Transplantation-Stats>. 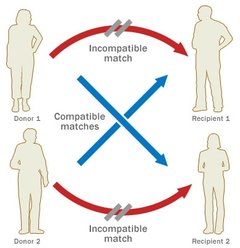 When the patient reaches end-stage renal disease they are usually faced with two options: dialysis or a transplant. Dialysis is the more common of the two, but transplants may keep the patient more free and independent. There are two main types of kidney procedures: deceased-donor and living-donor transplants.
A healthy individual has the option to donate his or her body when they die, and the kidneys are often utilized in transplants. Once the kidney is removed from the deceased body, it is either iced immediately, or is kept on a machine that pumps oxygen into the tissues so it may remain healthy and fresh. Either way, it is crucial that the kidney does not travel very far, because the more time spent outside a living body the worse it may become. Contrary to popular belief, a patient with end-stage renal disease only needs one kidney, so thankfully resources may be saved. The non-functioning kidney still remains in the body, and the new kidney is placed in the front of the stomach, opposed to the back. This seems like a much better option than dialysis, because the patient doesn’t have to spend 12 hours a week in the clinic. However it is difficult to find a match for a patient, due to the lack of compatibility and registered donors. About two thirds of transplant patients receive kidneys from deceased donors, whereas the others mostly come from live donors. Generally speaking, living-donor kidneys do much better than deceased kidneys. For one, the kidney lasts longer both in the short term and the long term. Deceased donor kidneys may also have delayed functions, whereas the living donor kidney starts working immediately. If you wanted to donate your kidney to a close friend or family member, it is important to know what makes a good “match.” No two individuals are the exact same: we each have different blood and tissue types. They do not have to be the exact same, but the blood must be compatible. For example, if the donor is blood type A, they are compatible with patients who have blood types AB and A. But even if you aren’t exactly compatible with the person you want to donate to, there is still a way for it to work! The transplant clinic may offer you and the patient a chance to do a paired donation. As shown in the diagram, your blood and tissue types are compared with other patients in the clinic, and if you can match with a patient who couldn’t match with their preferred donor, the two donors may “trade” kidneys to make both patients happy. Donors are unfortunately very scarce, but due to the amount of people needing kidneys, you will most likely find a patient that matches with your kidney, so it will not be wasted. Sources: Mayo Clinic Staff Print. "Kidney Transplants." Mayo Clinic. N.p., 24 June 2016. Web. 03 Apr. 2017. <http://www.mayoclinic.org/tests-procedures/living-donor-kidney-transplant/pdc-20207271>. "Organ Donation: Demand versus Supply." ExpatHealth.org. N.p., n.d. Web. 03 Apr. 2017. <https://expathealth.org/healthcare-news/organ-donation-demand-versus-supply/>. |
